
Multiple Sclerosis (MS) is the most common inflammatory demyelinating disease that affects different areas of the white matter of the brain and spinal cord. In its most common clinical form (relapsing-remitting MS), is characterized by recurrent attacks which in the early stages of the disease tend to regress completely, but that with the passage of time hesitate in accumulation of disability. The disease has a strong social impact by its spread and tend to affect people of young age. And it’s the first cause of disability in young adults after trauma skull-bone marrow.
Clinical presentations are represented by loss of strength and / or susceptibility to a limb, retrobulbar optic neuritis.
The symptoms of advanced stage are composed of serious force and psychics deficits, spasticity, coordination disorders, visual impairment, cognitive and behavior impairment .
At present there are many drugs used for both treatment and relapses, both in an attempt to modify the course of the disease. Treatment with high-dose steroid (1 gr / day x 5-10 days) is indicated only in case of relapse.
Among the immune-modulating therapies which modify the course of the disease, Interferon beta (IFN-beta) is able to reduce the risk of relapses by 30-40%, only slightly slows down the progression of the disease and reduces the number of active lesions at the Magnetic Resonance (1-2).
The so-called biological drugs, monoclonal antibodies, have come to the fore in recent years and the Natalizumab was the first to be used . It reduces by 70% the rate of relapse, 80-90% of the number of active lesions visible on MRI, and 40% of disability progression (3-4-5). And it’s well-it tolerated during the first year of treatment, but in the second year it was associated with the onset of severe encephalitis with a frequency on the whole rare 1/1000.

In this area of the clinic very delicate and demanding therapies Complementary and Alternative Medicine (CAM), they have been proposed for the treatment of the symptoms of the disease as adjuvants of irreplaceable traditional therapies. A study carried out in California and Massachusetts shows that 60% of MS patients use alternative medicine (6-7-8).
Indice dell'articolo
Nutritional aspects
A brief mention should be made also to the nutritional aspects that play a significant role in disease management.
An investigation lasting 34 years and started in 1949 was carried out by American neurologist Roy Swank, whose results were published in “American Journal Nutrition” in 1988, and then on “Lancet” in 1990.
It involved 150 patients with multiple sclerosis who have been fed a diet low in saturated fat not more than 20 grams. per day. Whole milk, cheese, margarine and other sources of hydrogenated fats have been abolished and there has been an integration with 5 gr. a day of cod liver oil (the main source of omega-3) and 5 to 40 g. / day of vegetable oils rich in polyunsaturated fatty acids.
The results after 34 years of follow-up have said that among the 70 patients who had adhered to the assumption of no more than 20 g / day of saturated fat mortality was 31% and the average degree of deterioration was minimal.
On the contrary among the 74 patients who had consumed more than 20 g / day of saturated fat, disability was severe and very frequent with the mortality rate risen to 80%. Slightly disabled patients who adhered to the diet showed none or minimal deterioration and 95% were still alive after 34 years, however, the interruption of the diet even after 5 or 10 years, was followed in almost all cases with reactivation of the disease. (9-10-11-12-13-14-15).
Two other more recent studies have shown the benefits of Swank diet. A first study published in “Scandinavian Neurological Acta” in 2000, was about 16 patients with multiple sclerosis whose recently duration was of 18 months and in which after two years of treatment, the mean annual relapse rate was 0.06 episodes per person compared to 1 , 39 recurrences per person prior to the study. The reduction was 96%. After two years , the degree of disability was reduced by 25% from baseline (16).
A second study published in “Prostaglandins Leukot Essent Fatty Acids” in 2005 on 31 patients with relapsing-remitting multiple sclerosis, after 11 months of treatment, the measure of physical functioning and mental health were significantly better in patients assigned to diet with low fat (15% of total energy) than those assigned to the diet with a fat content equal to 30% of the total energy (17).
There are epidemiological studies correlating intake of cow’s milk and the onset of multiple sclerosis (18-19). These researchers found a very high correlation between milk consumption and onset of the disease.
The fact is that in clinical practice outpatient discontinuation of milk in these patients more often than you might think, leads to marked improvement by increasing the time between relapses.
Natural treatment with herbs and spices
The plant compounds that have shown some action on the inflammatory process of MS are essentially turmeric, green tea and some classes of flavonoids.
Even in the “natural” there are herbs and spices that can be potentially harmful to the disease and it is good to have some information on this topic.
Plants potentially harmful
- Some plants such as Echinacea, Astragalus and Spirulina should be avoided in a systemic immune disease such as MS, as possessing immunostimulant which could aggravate its evolution (20-21-22).
- Tiredness and fatigue is one of the most common disorders in MS patients which often use energy enhancers or stimulants natural based. Plants such as tea, coffee and guarana which contain caffein and cola and also Citrus aurantium (bitter orange) and Ephedra (ephedrine) could be harmful and worsen symptoms due to their stimulating properties on the central nervous system.
- The American ginseng does not improve fatigue in Multiple Sclerosis and therefore is to be avoided (23).
- Gingko biloba does not improve cognitive performance in multiple sclerosis and it is to be avoided (24-25).
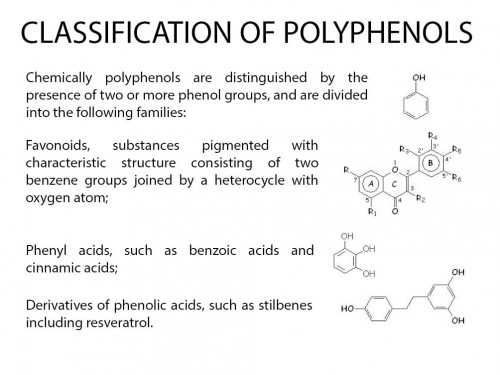
Polyphenols
Polyphenols are classified into four categories: phenolic acids, flavonoids, stilbenes and lignans with flavonoids, which are further classified into six subclasses. They are products intensely studied for two decades due to their ability to improve human health.
Flavonoids possess three properties that make them very useful in neuroprotection.
- They are very powerful antioxidants and versatile, they are able to neutralize the radical “peroxynitrite” particularly destructive in neurodegenerative diseases (26-27).
- They are potent inhibitors of dangerous lipid peroxidation products that are found in high concentrations in Alzheimer’s disease, Parkinson’s disease and Amyotrophic Lateral Sclerosis (28).
- They avidly bind iron, copper and other neurotoxic metals (29).
They are found in fruits and vegetables, especially abundant in grapefruit, in tea,in olive oil and in red wine. (30) They have several functions: antioxidant, anti-allergic, anti-cancer and anti-inflammatory. There are more types but those who have shown some activity against SM are quercetin, luteolin, curcumin and green tea.

Luteolin
The Luteolin is a regulator of the immune system, it can be effective in certain neurodegenerative diseases such as Multiple Sclerosis going to inhibit the inflammatory process. It is located in the artichoke leaves, rosemary, thyme and chamomile.
In an interesting article by Sternberg appeared in the “Journal Neuroimmunology” in 2008 it is shown as the Luteolin inhibits the release of inflammatory substances such as interleukin 1 and TNF (tumor necrosis factor), by activated macrophages in peripheral blood of patients with multiple sclerosis (31) . Moreover, the effect of the substance is enhanced by concomitant administration of IFN-beta, a powerful drug commonly used immune-modulating treatment clinic (32).
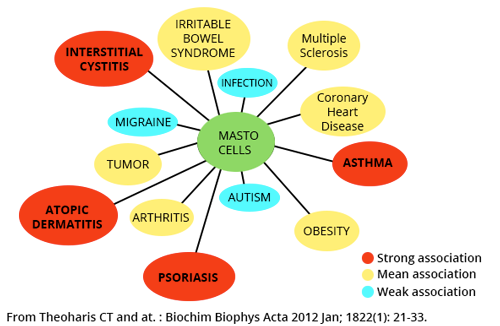
Mast cells are cells known for a long time now for their intervention in allergic reactions and in anaphylactic shock. Recent findings indicate that these cells are also found in the vicinity of neurons and are the link between the immune, endocrine and nervous system playing an important role in access to pathogens and lymphocytes to the brain (33). These cells are considered to be the next target in the treatment of multiple sclerosis (34-35).
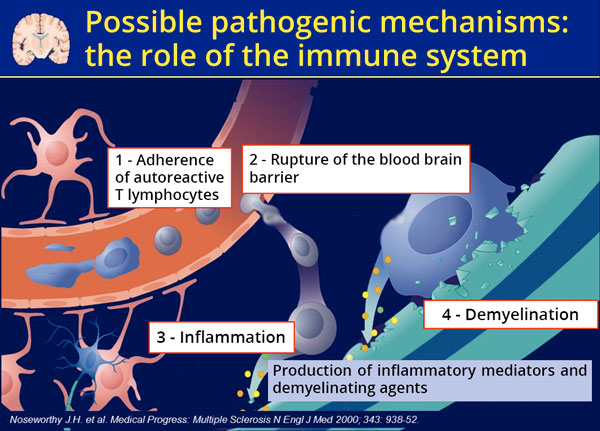
Luteolin inhibits the release of inflammatory substances from the “mast cells” which play an important role in the development of the disease having the power to form areas of cerebral demyelination (nerve cells with damaged myelin conduct impulses more slowly). Furthermore luteolin prevents the passage of pathogens and lymphocytes from the blood to the brain. The “tightness” of the important blood-brain barrier undergoes profound changes during the illness becoming permeable and allowing the spread within the nervous system of cellular elements that can trigger damage on the myelin membrane of neurons (36-37-38).
It ‘s a substance so studied and so interesting that it has already received three US patents covering the use of flavonoids in inflammatory diseases, also there are patent applications specific to the combination of luteolin and INF-beta for the treatment of Multiple Sclerosis (39).
Luteolin: therapeutic hypothesis
The Luteolin must be taken at doses of at least 100 mg / day to twice a day, morning and evening, during the classic pharmacological therapies for long periods.
Very important it is the association with turmeric which enhances and completes the action (see below).
Quercetin
Quercetin is a major flavonoid and one of the most potent antioxidants plant . The consumption of flavonoids and quercetin in particular, is associated with a reduced risk of coronary heart disease and degenerative diseases. (40-41-42-43-44-45). The daily intake with a typical Occidental diet amounts to 10-30 mg with an average of 10 mg daily doses are far from “drug” that amount to more than about 500 mg, necessary to counter a neurodegenerative process such as Multiple Sclerosis.
And it’s interesting to note that the largest amount of quercetin is found in capers at a concentration of 233 mg / 10 g, followed by cocoa powder with 22 mg / 100 g (46).
Quercetin improves endothelial function with independent mechanisms by nitric oxide (NOS) (47) . It has anticoagulant properties thanks to its ability to bind competitively to the plasminogen which in activating plasmin, allows the dissolution of the clot (48-49). It has an antiproliferative effect on smooth muscle cells of the small arteries favoring arteriolar dilation and low blood pressure (50-51). It reduces ventricular hypertrophy and programmed death (apoptosis) of the heart muscle cells (myocytes) (52-53).
In a paper published in “Life Science” in 2010, Quercetin has been shown to decrease inflammatory responses and provide neuroprotection by inhibiting the production of NO (nitric oxide) and INF-gamma by microglial cells (54-55), it also prevents inflammatory cytokine impiding neuronal damage (56-57). In another work published in “Journal Neuroscience Research” in 2008, along with Resveratrol and Quercetin it has been shown that it is possible to reduce neuronal death by apoptosis (programmed cell death) induced by neuro inflammation (58).
There are encouraging data that show protective effects of polyphenols in both animal models and in vitro relevant multiple sclerosis (59). Quercetin has been reported to be effective in mouse model of “experimental autoimmune encephalomyelitis,” in reducing the proliferation of T lymphocytes in vitro at high concentrations (60).
Having played a very accurate model of multiple sclerosis in animal models has been crucial to understanding the mechanisms of the disease (61). The « Experimental Autoimmune Encephalomyelitis” of the mice mice is the model that most of all the other reflects the pathogenesis of multiple sclerosis in human beings and is extremely useful for studying potential experimental treatments (65-63). In other words, a treatment that does well in this model has a good chance to be active also in humans.
The studies available nowadays show that the polyphenols have the ability to suppress the immune and inflammatory responses in animal models of multiple sclerosis (64-65).
Quercetin: therapeutic hypothesis
The concentration of quercetin in plasma varies greatly with age, sex and type of activity. In a challenging disease like multiple sclerosis dosages should go from 500 to 1000 mg per day given twice daily morning and evening for three-month cycles (66-67-68).
Excellent combination of Quercetin and Luteolin.
Morning: 500 mg of Quercetin and 100 mg of Luteolin.
Evening: 500 mg of Quercetin and 100 mg of Luteolin.
Turmeric
Turmeric through its main compound, Curcumin, has a strong anti-inflammatory effect (69). It has been well documented over the past decade that inflammation plays a role in most of the chronic diseases such as neurodegenerative, cardiovascular, autoimmune and cancer (70). In all these conditions curcumin has been shown to have a high therapeutic action going to inhibit an impressive series of molecular targets that are thirty according to a work published by Aggarwal in ‘”International Journal of Biochemistry & Cell Biology” 2009 (71).
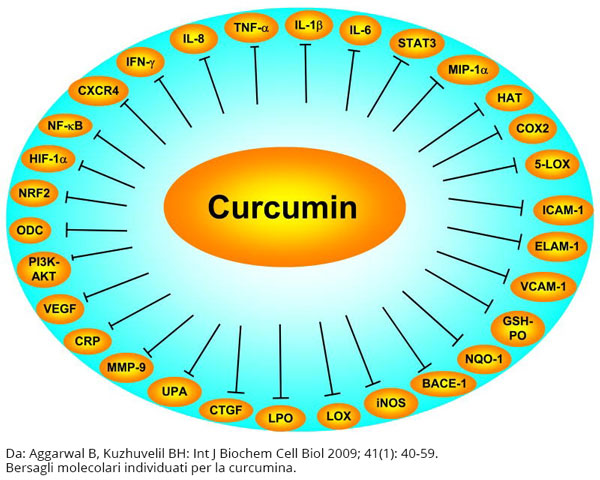
Among the most important there is the inhibition of the synthesis of nuclear factor (NF-kB) which has a central role in the control of inflammatory response both in tumor development : in fact it stimulates cell growth and inhibits apoptosis (programmed suicide).
The formation of this protein is closely related with the majority of chronic diseases and cancer, and agents which are able to suppress it are actively sought in laboratories around the world. The first that has shown that curcumin is a potent inhibitor of the activation of NF-kB was Aggarwal in 1995 in an article in the “Journal Biological Chemistry” (72-73).
Despite not having clinical trials available, we have the experimental tests, both in vitro and in vivo, which attest the neuroprotective properties of turmeric on multiple sclerosis (74). In a work published in the “Journal Immunology” in 2002, it is proven that curcumin significantly reduces the duration and clinical severity of experimental allergic encephalomyelitis in animal models going to reduce the production of Interleukin -12 (IL-12), proinflammatory cytokine that plays a crucial role in the induction of the disease (75-76-77).
A series of recent studies have provided evidence that the T-helper cells that produce interleukin-17 (IL-17), have a central role in the development of Experimental Autoimmune Encephalomyelitis. Treatment with curcumin significantly reduces the clinical severity of the disease, the infiltration of inflammatory cells into the spinal cord and the proliferation of activated lymphocytes against myelin protein (MBP lymphocytes). These results indicate that curcumin may be useful in the treatment of multiple sclerosis and other inflammatory Th-17 cell-mediated (78-79).
Turmeric: therapeutic hypothesis
Meriva’s Turmerichas a high intestinal absorption, also available in dosage form in numerous pharmacies:
1 cps 500 mg. After breakfast
1 cps 500 mg. After dinner
Turmeric possesses no dose-limiting toxicity at least 12 grams / day orally. In clinical studies on pancreatic cancer, they have been used up to 8 grams per day of spice (80-81-82-83-84). With the formulation Phytosome (Meriva) is it possible to obtain absorptions 10 times higher and then at a dose between 1 and 2 grams per day it is assured an optimal plasma level for the action of the spice.
The problem is not the administration of high doses, but it is the study of the association between spices which greatly increases the effectiveness for a natural and spontaneous synergy.
Important association with other spices.
The rationale of the association of turmeric together with the Luteolin is derived from the fact that the latter tends to prevent the passage of inflammatory cells at the level of the blood-brain barrier and turmeric amplifies this action by inhibiting the formation of TNF (Tumor necrosis factor) (85 -86-87) that plays an important role during permeabilization disease (88-89-90-91).
I remember that natalizumab as prime function, it blocks cell adhesion and prevents the migration of leukocytes through the blood-brain membrane with arrest of the inflammatory process.
Combination therapy
Turmeric 1 cps 500 mg + 1 cps luteolin 100 mg after breakfast
Turmeric 1 cps 500 mg + 1 cps luteolin 100 mg after dinner
Green tea
Green tea contains a series of compounds, called catechins, which play a marked neuroprotective action in the brain. As curcumin and other flavonoids, extracts of green tea have a strong antioxidant and anti-inflammatory action, they suppress excessive immune response, neutralize metals and play anticarcinogenic actions (92-93), also its constant consumption is inversely related to the incidence of dementia, Alzheimer’s disease and Parkinson’s disease.
In a recent clinical trial published in “American Journal Clinical Nutrition” in 2015, it is studied in 18 patients suffering from relapsing-remitting MS, the metabolic muscle response during moderate exercise, to the administration of 600 mg / day of epigallocatechin-gallate ( EGCG), the active ingredient in green tea.
The trial had as final goal of improving the study of fatigue and muscle weakness, very common and disabling symptoms during illness. The results showed an improvement in muscle metabolism and the above parameters more in men than in women because of gender-specific effects such as hormonal (94).
Very interesting news are coming from studies on sperimental auto – immune encephalomyelitis on animals in which the administration of the substance reduces the severity of the disease by reducing inflammation and brain damage from the loss of myelin. In a work of Chinese school appeared in the journal “Front Biosci”, 2013, it is clarified that some mechanisms of action of epigallocatechin-gallate which in this disease must be used at high doses (from 800 mg up) effectively becoming a “drug” capable of inhibiting substances highly inflammatory molecules such as Interferon-gamma and interleukin-17, in addition to performing the particular action to selectively inhibit some pathogenic clones of autoreactive lymphocytes (95-96).
Also in another study published in the “Journal Immunology” 2004 it is shown for the first time that EGCG plays an inhibiting action both on the formation of the nuclear factor NF-kB (97) and on the production of free radicals that are so important in the processes of neurodegeneration and neuroinflammation (98).
Green tea: therapeutic hypothesis
The dosages of epigallocatechin-gallate (EGCG) are ranging from 400 to 1200 mg / day divided into two daily doses.
An helpfuldosage in multiple sclerosis is 400/600 mg morning and evening preferably associated with curcumin.
Morning: 1 cps (EGCG) 400 mg + 1 tablet 500 mg curcumin
Evening: 1 cps (EGCG) 400 mg + 1 tablet 500 mg curcumin
Curcumin and EGCG have in common (along with other natural substances) the inhibition of nuclear factor NF-kB, a very important element for the development of any neuro inflammatory process, their association develops an inhibitory synergy much more striking.
A triple combination in difficult and worsening cases involves the use of Luteolin in addition to the usual dose of 200 mg / day divided into two doses at meals.
Associations
Morning: 1cps (EGCG) 600 mg + 1 tablet 700 mg curcumin
Evening: 1 cps (EGCG) 600 mg + 1 tablet 700 mg curcumin
Lunch: 1 tablet 100 mg luteolin.
Dinner: 1 tablet 100 mg luteolin
Another triple combination which can be used as an alternative to that one , involves the use of Quercetin in place of Luteolin:
Morning: 1 cps (EGCG) 400/600 mg + 1 tablet 500 mg curcumin
Evening: 1 cps (EGCG) 400/600 mg + 1 tablet 500 mg curcumin
Lunch: 500 mg Quercetin
Dinner: 500 mg Quercetin
Conclusions
On the usefulness and effectiveness of alternative unconventional therapies (CAM) for multiple sclerosis, there is a significant gap of opinions among patients who use it and doctors with traditional views.
In fact, we must admit that there is a significant shortage of well designed clinical trials that assess the benefits of CAM for multiple sclerosis, but the lack of evidence does not mean no benefit!
We have to identify CAM therapies that have some rationale for the wellness of patients and we must plan and design new experiments to determine what works and what does not.
As shown in this study , the evidences justify an experimental study around these spices, substances associated with conventional therapies in many patients loose the “virulence” of the disease allowing relapses occur with larger time intervals.
When you consider the proven safety and large tolerability of such substances , I see no reason to oppose the attempts of those who seek other “escape routes” in addition to the traditional ones, especially given the complementarity of interventions.
In our small outpatient series , we had a very challenging case of a girl whose cycles in treatment with natalizumab developed a relapse every 3-4 months showing a motor deterioration and gradual worsening. After adding to traditional treatment, the three above-mentioned association composed of curcumin, epigallocatechin-gallate and luteolin at high doses, in a year since the crisis is yet to resubmit a relapse , all on time continuing treatment with the monoclonal antibody.
Taken as a “case report” it is interesting and it deserves a deepening through the recruitment of other patients from colleagues and comparing data after some time, but it must be admitted, unfortunately, that time is not yet ripe.
Dott. Claudio Sandri
Translated by Ms Jeanne Marie Arcaini
Bibliography
Article bibliography at the following link.